


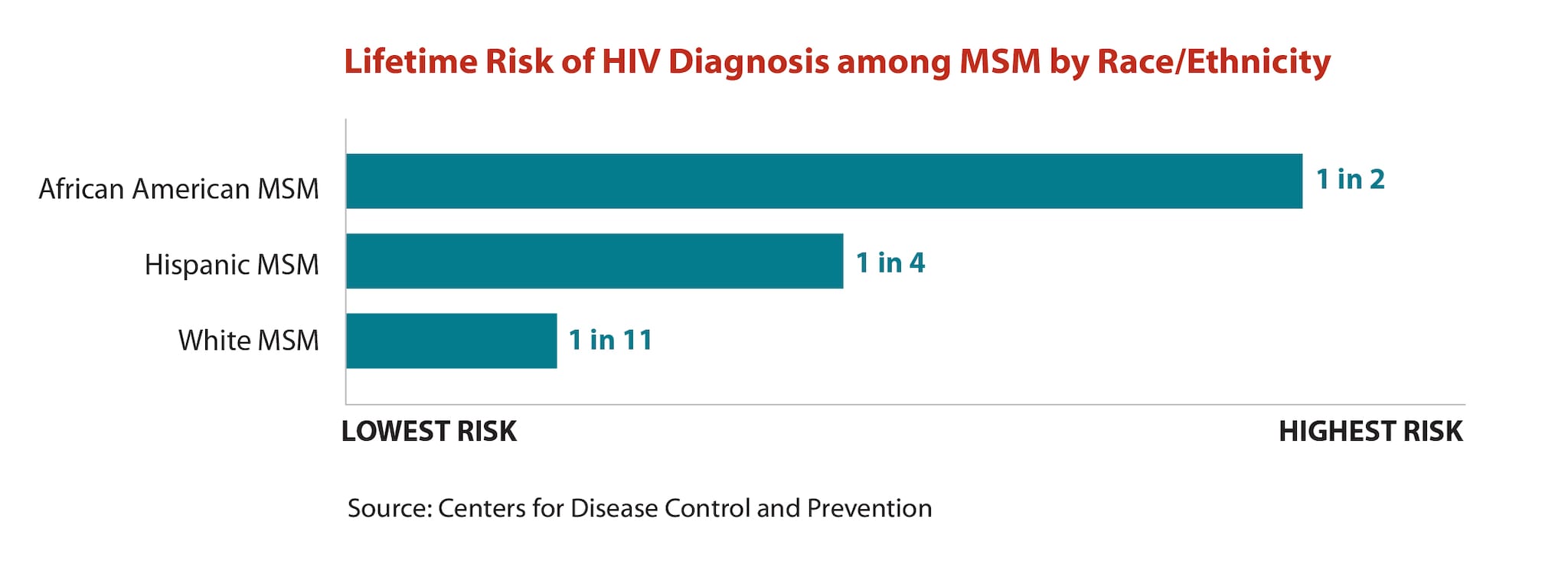
Amid disproportionate gains in HIV prevention, half of gay black men and a quarter of gay Latino men are expected to contract the disease in their lifetimes.
By Elena Gooray
A man has blood drawn to test for sexually transmitted infections. (Photo: Stephen Chernin/Getty Images)
We’re making progress on fighting the HIV/AIDS epidemic — just not fast enough, according to White House-set standards, especially among the groups most vulnerable to the virus.
Over the past five years, the number of new HIV infections occurring annually has dropped by an estimated 11 percent, and the overall transmission rate — the number of new cases per person living with HIV — has decreased by an estimated 17 percent, according to research published last week in AIDS and Behavior. While those reductions are good news, they fall short of the goals set by President Barack Obama’s 2010 National HIV/AIDS Strategy (NHAS), which sought greater blows against the epidemic by the end of 2015. The targets sought to decrease the number of new infections by 25 percent, and the transmission rate by 30 percent.
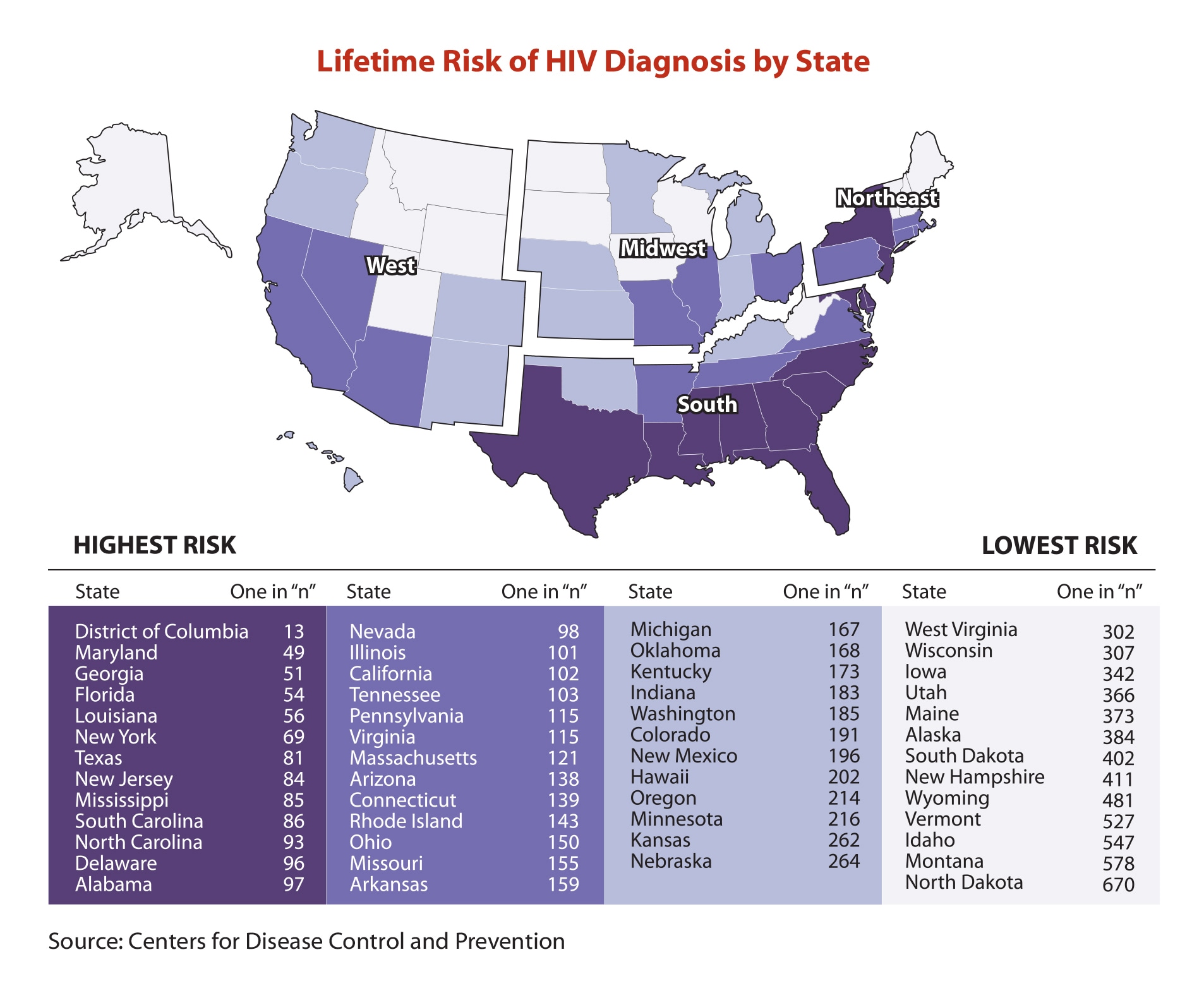
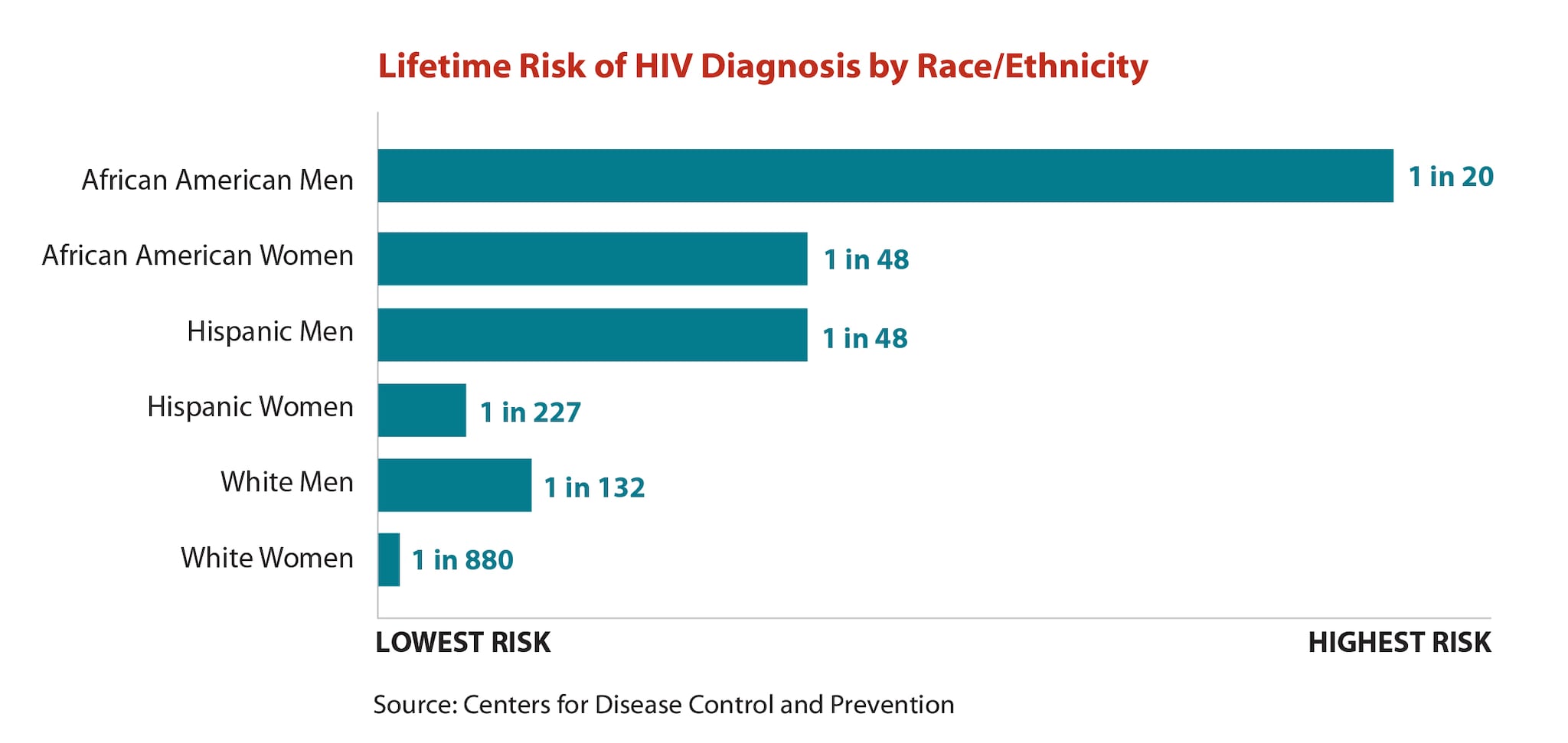
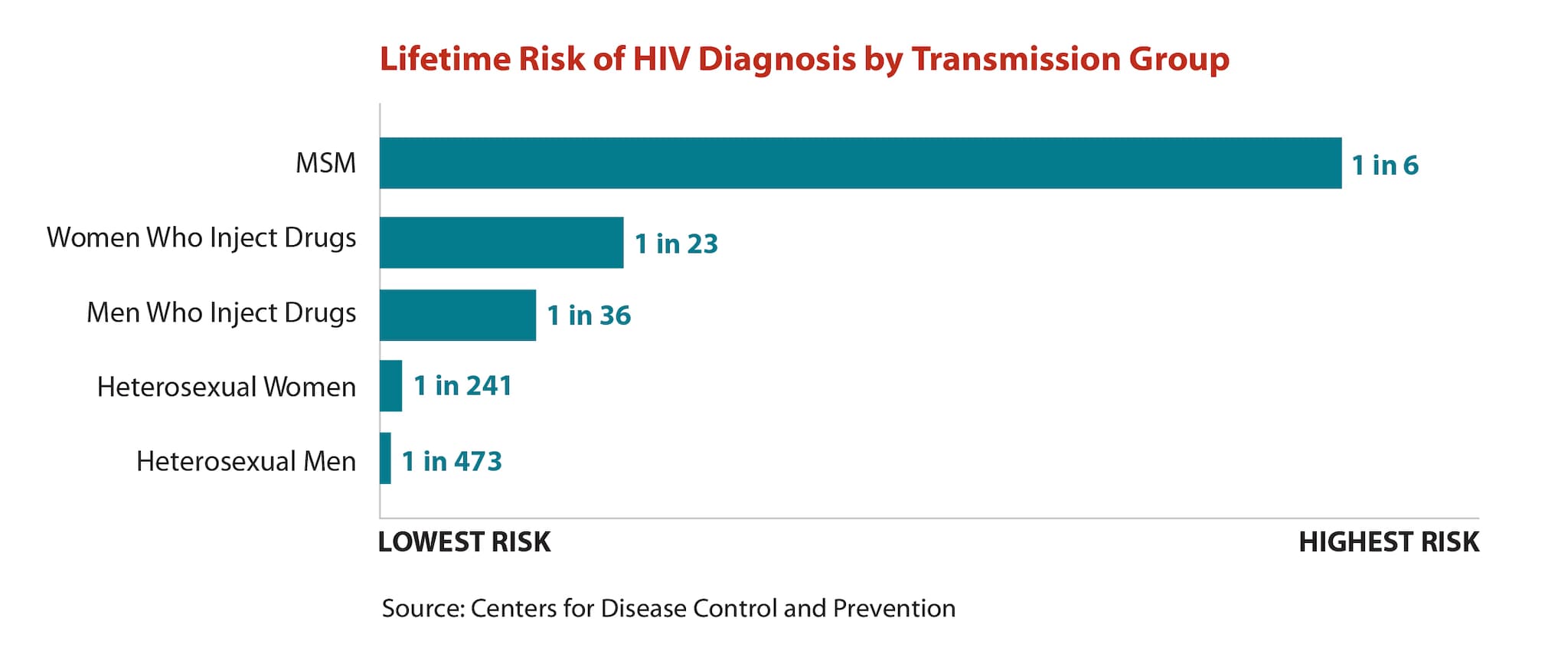
This evaluation of the NHAS impact comes just two months after a report from the Centers for Disease Control and Prevention (CDC) that found half of gay black men, and a quarter of gay Latino men, are projected to be diagnosed with HIV within their lifetimes. HIV continues to disproportionately affect specific (though overlapping) populations — youth ages 13 to 24, transgender women, residents of Southern states, those living in urban poverty, and black and Latino men and women. Gay and bisexual men remain the broad demographic group most likely to be diagnosed with HIV, with black and Latino men in that group at the greatest risk.
“We feel really positive that the HIV incidence rate seems to be dropping.”
The recent AIDS and Behavior research highlights the parallel, conflicting narratives of our fight against the epidemic: On one hand, infection rates are decreasing, but not all Americans are seeing equal benefits of that downturn.
“We feel really positive that the HIV incidence rate seems to be dropping,” says Robert Bonacci, lead author on the AIDS and Behavior study. This change follows 25 years of worrying trends — an increase in new HIV cases during the mid- to late-1990s, a slight decline after 1999, and stagnant rates since then. The White House strategy came in the wake of that stagnation, and Bonacci’s assessment of CDC data suggests that post-2010 efforts have broken through that plateau.
But those gains have most strongly transferred to straight Americans, people who inject drugs, and black women (relative to black men). To reach other populations, Bonacci says, HIV reduction efforts should focus as much on diagnostic testing and prevention as on treatment for those already living with the disease, which has received the bulk of recent federal budget increases. Adequate treatment can help prevent transmission by reducing the number of HIV particles in people’s bodies to lower levels, reducing their risk of passing on the disease. But high-risk populations also need increased access to pre-exposure prophylaxis, or PrEP, a daily pill found to reduce HIV transmission among gay and bisexual men by at least 44 percent. These groups can also benefit from increased use of condoms, which reduce the risk of infection by at least 90 percent when used consistently.
Although we are currently trailing the NHAS goals — which have since been revised and extended to 2020 — the strategy still creates a useful timeline for combating HIV, according to Bonacci. “They set high [progress] levels to inspire our communities to be ambitious about taking on the HIV epidemic,” he says. “And setting this timeline allows us, every five years, to re-evaluate our progress and re-adjust the strategy to really make an impact.”
Bonacci and his co-author, David Holtgrave — who published an editorial Tuesday in the Huffington Posturging the next presidential administration to set HIV prevention goals — had to use data from 2010 to 2012 to project transmission reductions from 2013 to 2015, since the CDC has not yet finalized data for those latter years. As a result, the recent study may have underestimated the progress made since 2010, if post-2013 prevention efforts in fact had a larger impact than those of the previous years. HIV data is constantly being updated as the CDC refines its collection, meaning another part of the strategy should involve more researchers assessing HIV data to compare results, Bonacci says.
Whatever gains we’re making, we need more researchers to monitor them — and to help bring that progress to those who need it most.

||



{kind=link}
{kind=link}
{kind=link}
{kind=link}